Oregon reported 1,388 COVID-19 deaths as of December 20, 2020.1 To understand the relevance of this number, it is important to have a solid understanding of how overall deaths from 2020 compare to historical data, how deaths are reported, what constitutes a COVID-19 death, and the accuracy of deaths reported.
Oregon Deaths per Year
Over the past 3 years, Oregon averaged 36,743 annual deaths2 with cancer and heart disease historically being the leading causes.3 As of December 20, 2020, Oregon has had 38,304 deaths with COVID-19 only accounting for 3.6% (1,388 / 38,304). The number of Oregon’s 2020 deaths is 3,167 more than the 3 year average for the same time range (this is known as excess deaths).4
What is extremely interesting is that COVID-19 only contributes 1,388 deaths (less than half) to the excess total. 1,779 of all excess deaths are from other causes and significantly started ramping up around the end of March. Further investigation is needed to determine the cause. Could suicide, inaccessibility to medical treatment, and overdose due to government lockdowns be contributing to these deaths?
“Cause of Death” Reporting
Beginning in 2003, all deaths in the United States have been reported based on the Medical Examiners’ and Coroners’ Handbook. The “cause of death” portion of a death certificate consists of Part I (with multiple lines) and Part II. Part I lists the immediate cause of death on the first line (a) and any conditions that led to the death (known as comorbidities) on subsequent lines (b), (c), and (d). Part II is used for listing any other diseases, conditions, or injuries that were present but did not contribute to the cause of death. Filling out a death certificate accurately is extremely important because Part I is used for public health reporting and death statistics. Data in Part II is rarely reported.5
For example, if someone were to die from a heart attack (myocardial infarction), this would be listed on the first line (a) of Part I. If the heart attack were due to coronary artery disease, this would be listed on the second line (b) of Part I. If the patient had a cough a few weeks prior to death warranting a H1N1 (swine flu) lab test which confirmed infection, it would be listed depending on its contribution to death. If the H1N1 infection were present, but did not impact the cause of death (myocardial infarction) then it would be listed in Part II. However, if the H1N1 infection did impact the cause of death, it would be listed on line (d) of Part I. The highest an infectious disease could be listed would be line (d) of Part I5 because people don’t die from the disease; they die from complications of the disease (like heart attack or pneumonia).

Figure 1. An example of how the “cause of death” section in a death certificate was written before COVID-19.
How COVID Death Certificates are Written
On March 24, 2020, the National Vital Statistics Systems (NVSS) changed the way death certificates are written when COVID-19 is either suspected or confirmed.6 While deaths from other infectious diseases are based on the 2013 Handbook, COVID-19 deaths are reported in a completely unprecedented way.
According to the NVSS policy change, COVID-19 should be listed as the immediate cause of death on the first line (a) of Part I “more often than not,” even if the deceased person had other significant comorbidities.5 All other comorbidities are to be listed in Part II (not Part I as before).Additionally, COVID-19 should be listed as the immediate cause of death, “where the disease caused or is assumed to have caused or contributed to death.” This new rule significantly changes the statistical significance of deaths listed as COVID-19, not only in Oregon, but in the entire United States as well.
How Easily COVID Deaths are Diagnosed
Historically, a positive lab test must confirm a pathogen’s presence in order to be listed definitively (not presumed) on a death certificate.5 On April 14, 2020, the Centers for Disease Control (CDC) and the National Institute of Health (NIH) adopted a paper written by the Council of State and Territorial Epidemiologists (CSTE).7 The CSTE position paper allows for two major changes when it comes to diagnosing someone with COVID-19.
First, a patient can be considered a “probable case” if they have coughed a single time along with being within 6 feet of a COVID-19 positive patient for a minimum of 10 minutes, or having traveled to an area with an outbreak.7 Second, contact tracers, who are not required to have any form of medical training, can report individuals to local health departments who meet the probable case definition for COVID-19.8,9 They can do so without giving an exam, seeing a patient in person, or even talking with the suspected person on the phone.7
This is an extremely important distinction regarding death certificate reporting because, if a person dies and has a COVID-19 diagnosis or meets the easily achieved criteria set by the CSTE paper, COVID-19 can be listed as cause of death on line (a) of Part I. A positive laboratory test is not required.
COVID-19: Dying From vs. Dying With
OHA spokesman Jonathan Modie explained, “We consider COVID-19 deaths to be deaths in which a patient hospitalized for any reason within 14 days of a positive COVID-19 test result dies in the hospital or within the 60 days following discharge.”10 Due to these changes in death reporting, there is no way to know if someone died from or with COVID-19. This, in addition to inaccurate COVID-19 PCR results, greatly inflates COVID-19 death reporting.11
Anyone who dies and was suspected of having COVID-19 (based on rules from the CSTE Position paper) or who had a positive lab test within the previous 60 days, more often than not will have COVID-19 listed as the immediate cause of death on Part I, line (a) of their death certificate, regardless of what actually killed them.
One such example happened in July 2020, when an Oregon man fell from a ladder and died due to sustained injuries. A post-mortem COVID-19 test came back positive. He was listed as a COVID-19 death by the OHA. Philip Schmidt, a spokesman for the OHA, told The Oregonian, “The state’s data is not conclusive as to whether someone died as a result of the coronavirus. Rather, it shows only that they died carrying the virus.”12
Death Certificates: COVID-Style
Let’s return to our original death certificate example where the patient died from a heart attack. Instead of using H1N1, COVID-19 will be used along with the new policy for completing death certificates. Our patient visited an area with an outbreak, still had a cough two weeks prior to their death, but no lab tests were performed. According to the new rules, COVID-19 would be listed on the first line (a) of Part I. Myocardial infarction would move down to Part II along with coronary artery disease. The death would be reported as COVID-19. Myocardial infarction or coronary artery disease might not even be reported by health authorities because only Part I is typically used.5 (See Figure 2 below.)
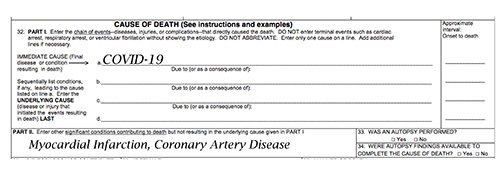
Figure 2. An example of how death certificates are now written. Same patient (from Figure 1) died from a heart attack and COVID-19 was suspected based on visiting an outbreak area and a cough two weeks prior to death (no lab test).
Comorbidities
Only 7 States (New York, Massachusetts, Georgia, Oklahoma, Utah, Pennsylvania, and Iowa) have reported data about comorbidities (other conditions that led to death) when publishing COVID-19 death certificates. According to data from these states, if death records had been done in the same manner as all other infectious diseases (the way it’s been done for the past 17 years), the total deaths from COVID-19 would be 90.2% lower than what is being reported.13
On May 12, 2020, OHA stopped reporting pre-existing conditions for COVID-19,14 making it impossible to verify accuracy of Oregon’s death data. To estimate how many people in Oregon died from COVID-19, not with COVID-19, we can use the other states’ data to extrapolate.13 If only 9.8% (100% — 90.2%) of deaths were caused exclusively from COVID-19, Oregon’s COVID death total would be 136, not 1,388 (.098 x 1,388). The remaining 1,252 (1,388-136) would have died with COVID-19 but from other causes. If you go back to our excess death number, 3,031 of the deaths (96%) would be from other causes. Extrapolation would be unnecessary if COVID deaths were reported as all other infectious diseases have been since 2003.
The CDC reported, “for 6% of the deaths, COVID-19 was the only cause mentioned. For deaths with conditions or causes (comorbidities) in addition to COVID-19, on average, there were 2.6 additional conditions or causes per death.”15 Italy came to a similar conclusion when studying COVID-19 deaths. They found that over 99% of those who died had pre-existing comorbidities.16
Even with overestimated death totals, COVID-19 mortality rates have significantly reduced since April. This means a smaller percentage of people who have been diagnosed with COVID-19 are dying. As of December 20, 2020, Oregon has a mortality rate of 1.3%, compared to 4.2% on April 28.20
Legal Implications
If you keep asking yourself if this could possibly be legal, in short, it’s not. The CDC is required to follow laws set by the Information Quality Act before making changes in death reporting.17 By altering the way death certificates are written and how COVID-19 can be diagnosed, they broke the law. All of the laws that were broken, policies ignored, and councils that were not notified are discussed in a peer-reviewed paper titled COVID-19 Data Collection, Comorbidity & Federal Law: A Historical Retrospective.18
Conclusion
Illegal policy changes allowed death certificates to no longer differentiate between dying from and dying with COVID-19. It is also possible that a COVID-19 diagnosis on a death certificate is merely a guess based on rules set by the CSTE position paper. Data gathered from death certificates can easily be used to mislead policy makers and the public.
How can our public health department and Governor make the best decisions for Oregon when given faulty data? Even with all of Oregon’s misleading COVID-19 deaths, we are ranked 39th in the country for COVID fatalities (as of December, 2020).19 Oregon is experiencing an increase in excess deaths with COVID-19 contributing to less than half of the total and only making up 3.6% of all deaths. We are seeing an explosion of COVID-19 cases (based on a flawed test) but a reduction in mortality rates. Cancer and heart disease continue to be the leading causes of death in Oregon.20 Where exactly is the emergency?
References:
- Oregon Health Authority. COVID-19 Updates. https://govstatus.egov.com/OR-OHA-COVID-19. Accessed 12/27/20.
- Oregon Health Authority. Oregon Death Data. https://www.oregon.gov/oha/PH/BIRTHDEATHCERTIFICATES/VITALSTATISTICS/DEATH/Pages/index.aspx. Updated 12/1/20. Accessed 12/27/20.
- Liz Meszaros. Top 10 causes of death in the US in 2020 https://www.mdlinx.com/article/top-10-causes-of-death-in-the-us-in-2020/MNpEowpA8DXKBUNcbmkpY. Published 2/27/20. Accessed 1/5/21
- Oregon Health Authority Center for Health Statistics. Weekly Deaths in Oregon https://public.tableau.com/profile/oha.center.for.health.statistics#!/vizhome/OregonHealthAuthorityCenterforHealthStatisticsWeeklydeathstable/Weeklydeathsummarydata. Updated 12/20/20. Accessed 12/31/20.
- Centers for Disease Control. Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death reporting. https://www.cdc.gov/nchs/data/misc/hb_me.pdf. Published 4/3/03. Accessed 12/27/20.
- National Center for Health Statistics. COVID-19 Alert No. 2: New ICD code introduced for COVID-19 deaths. https://www.cdc.gov/nchs/data/nvss/coronavirus/Alert-2-New-ICD-code-introduced-for-COVID-19-deaths.pdf. Published 3/24/20. Accessed 12/27/20.
- Council of State and Territorial Epidemiologists. Standardized surveillance case definition and national notification for 2019 novel coronavirus disease (COVID-19). https://cdn.ymaws.com/www.cste.org/resource/resmgr/2020ps/Interim-20-ID-01_COVID-19.pdf. Accessed 12/27/20.
- Centers for Disease Control and Prevention. Data Management for Assigning and Managing Investigations. https://www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tracing-plan/data-management.html. Accessed 12/27/20.
- Centers for Disease Control and Prevention. Notification of Exposure: A Contact Tracer’s Guide for COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/php/notification-of-exposure.html. Accessed 12/27/20.
- Severance C. Are dying with COVID-19 and dying from COVID-19 the same thing? In Oregon, they are. https://www.kgw.com/article/news/investigations/questions-over-the-accuracy-of-how-the-state-tracks-covid-deaths/283-0b1b7b6c-695e-4313-92cf-a4cfd7510721. Published 8/7/20. Updated 8/8/20. Accessed 12/27/20.
- Oregonians for Medical Freedom. PCR Tests Unraveled. https://www.oregoniansformedicalfreedom.com/2020/12/pcr-tests-unraveled/. Published 12/10/20. Accessed 12/27/20.
- Dole B. State officials reported Hermiston man as Oregon’s 226th coronavirus death. His family says they’re wrong. https://www.oregonlive.com/coronavirus/2020/07/state-officials-reported-edward-griggs-oregons-226th-coronavirus-death-his-family-says-theyre-wrong.html. Published 7/28/20. Accessed 12/27/20.
- Ealy H, McEvoy M, Sava M, et al. If COVID Fatalities Were 90.2% Lower, How Would You Feel About Schools Reopening? https://childrenshealthdefense.org/news/if-covid-fatalities-were-90-2-lower-how-would-you-feel-about-schools-reopening/. Published 7/24/20. Accessed 12/27/20.
- Oregon Health Authority. COVID-19 Weekly Report. https://www.oregon.gov/oha/PH/DISEASESCONDITIONS/DISEASESAZ/Emerging%20Respitory%20Infections/COVID-19-Weekly-Report-2020-05-12-FINAL.pdf. Published May 12, 2020. Accessed 12/27/20.
- National Center for Health Statistics. Weekly Updates by Select Demographic and Geographic Characteristics. https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm#Comorbidities. Updated December 23, 2020. Accessed 12/27/20.
- Istituto Superiore Di Sanita. Report sulle caratteristiche dei pazienti deceduti positivi a COVID-19 in Italia. https://www.epicentro.iss.it/coronavirus/bollettino/Report-COVID-2019_17_marzo-v2.pdf. Updated 3/17/20. Accessed 12/27/20.
- Office of the Law Revision Counsel. 44 USC 3516: Rules and regulations. https://uscode.house.gov/view.xhtml?req=granuleid:USC-prelim-title44-section3516&num=0&edition=prelim. Published 10/3/20. Accessed 12/27/20.
- Ealy H, McEvoy M, Chong D, et al. COVID-19 Data Collection, Comorbidity & Federal Law: A Historical Retrospective. Sci, Pub Health Pol, and Law. 2020;2:4-22. https://cf5e727d-d02d-4d71-89ff-9fe2d3ad957f.filesusr.com/ugd/adf864_165a103206974fdbb14ada6bf8af1541.pdf. Accessed 12/27/20.
- Elflein J. Number of deaths from coronavirus (COVID-19) in the United States as of December 22, 2020, by state. https://www.statista.com/statistics/1103688/coronavirus-covid19-deaths-us-by-state/. Published 12/22/20. Accessed 12/27/20.
- 2020 covidUSA. Oregon COVID-19 Statistics. https://covidusa.net/?state=Oregon. Updated 12/28/20. Accessed 12/28/20.